
Infectious Diseases
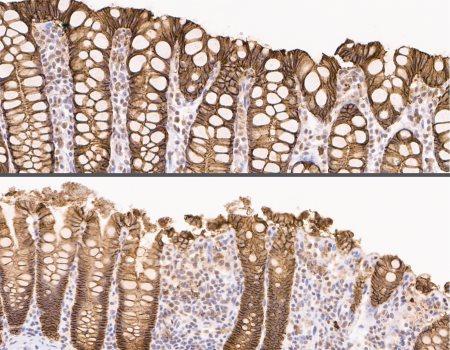 Cross sections of the large intestine of a control animal (top) and an animal with experimentally induced intestinal dysbiosis (bottom). Photo credit NIAID Cross sections of the large intestine of a control animal (top) and an animal with experimentally induced intestinal dysbiosis (bottom). Photo credit NIAID
Q&A: HIV and the Gut Microbiome
The gut microbiome—the community of bacteria and other microbes naturally present in the gastrointestinal (GI) tract—plays a critical role in human health. NIAID Now spoke with Jason Brenchley, Ph.D., about the link between the gut microbiome and HIV infection, and his lab’s recent research findings. Dr. Brenchley is senior investigator of the Barrier Immunity Section in NIAID’s Laboratory of Viral Diseases. What is gut dysbiosis? Is it common in people living with HIV? “Dysbiosis” refers to an alteration to the types of bacteria that normally inhabit the GI tract. Studies in humans have shown that the gut microbiome is dysbiotic in people living with HIV. This dysbiosis is associated with decreases in a type of bacteria that provides nutrients important for maintaining the health of the structural barrier of the GI tract, which prevents the microbiome from coming into direct contact with the GI tissues. When these bacteria are depleted in the case of HIV, the tight structural barrier of the GI tract weakens. The consequence of that is that microbial products cross the barrier into the tissues, where they can enter the bloodstream and cause systemic, or whole-body, inflammation. We refer to this as “microbial translocation.” Recent research suggests that a large degree of the gut dysbiosis observed in people living with HIV is not caused by the virus itself. Rather, gut dysbiosis may result from behaviors or risk factors associated with susceptibility to HIV infection. How can animal models help us better understand the link between gut dysbiosis and HIV? Animal models have certain advantages over human studies in that we can control for different variables that influence the composition of the gut microbiome—for example, diet. Using a non-human primate (NHP) model, we can follow the composition of the gut microbiome over time before and after infection with simian immunodeficiency virus (SIV), a virus similar to HIV. Your lab published a study today in Nature Medicine describing experimental induction of intestinal dysbiosis in monkeys infected with SIV. What was the focus of that study? The question we asked was: How does HIV-like gut dysbiosis change the nature of progressive SIV infection in our NHP model? We gave the animals an antibiotic that kills off many barrier-protecting gut bacteria, resulting in a dysbiotic microbiome very similar to that observed in people living with HIV. We infected the animals with SIV and followed disease progression over time. We also followed a control group of SIV-infected animals that did not receive the antibiotic. What were your main findings, and what do they tell us about the situation in people living with HIV? The dysbiotic microbiome that we induced had very little influence on how the disease progressed in the absence of antiretroviral therapy (ART). We measured multiple aspects of disease progression in the antibiotic-treated and control animals. We measured how well SIV replicated. We measured how quickly CD4+ T cells—the main cell type that SIV and HIV infect and destroy—were lost. We measured the degree of systemic inflammation and microbial translocation. None of those were altered by the dysbiotic microbiome. Assuming these effects are similar in people, our findings suggest that very little of the systemic inflammation seen in people living with HIV who are not on ART is attributable to gut dysbiosis. In the absence of treatment, immune responses to the replicating virus and translocated microbial products are likely the main cause of systemic inflammation. Is systemic inflammation also an issue for people living with HIV who are taking life-saving ART? Yes. Compared to the general population, people living with HIV who have been taking ART for decades are more likely to die from conditions associated with inflammation, such as cardiovascular disease and different kinds of cancers. Research suggests that much of the systemic inflammation seen in people whose HIV is suppressed by long-term ART stems from the phenomenon of microbial translocation, which may be linked to gut dysbiosis. What are the potential clinical applications of your research? There are two areas in which we think targeting a dysbiotic microbiome might be important for HIV. One is for reducing the risk of HIV acquisition. We are investigating whether gut dysbiosis changes susceptibility to HIV infection. In other words, if you have a dysbiotic microbiome, does that make it easier for you to acquire HIV? Some of our preliminary data suggests this may be the case. If you could increase the amount of good bacteria that are lacking in people at risk for HIV, it might make it harder for the person to acquire HIV. The other potential application is for people on ART who have residual inflammation. Developing strategies to alter their gut microbiomes to a less dysbiotic state might lead to them having lower levels of systemic inflammation and reduced susceptibility to cardiovascular disease and cancers. Source: niaid.nih.gov |
|